Post-partum mass in the uterine cavity

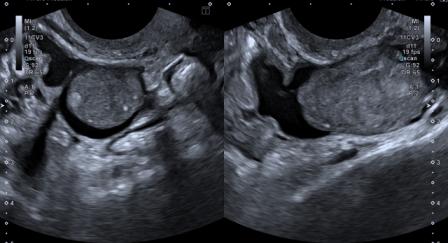
A 34-year-old woman (gravida 1, para 1) underwent cesarean section for fetal breech presentation. On post-partum day 27, the patient experienced bleeding per vaginum. Transvaginal ultrasound examination revealed an echogenic mass within the uterine cavity, measuring 45 x 25 mm. The ultrasound features were as follows:
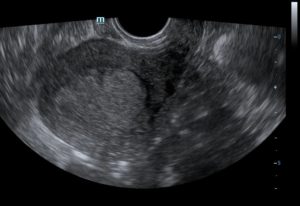
Figure 1: A hyperechoic well-defined mass in the uterine cavity. The interface between the mass and wall of the uterine cavity is distinctly defined.
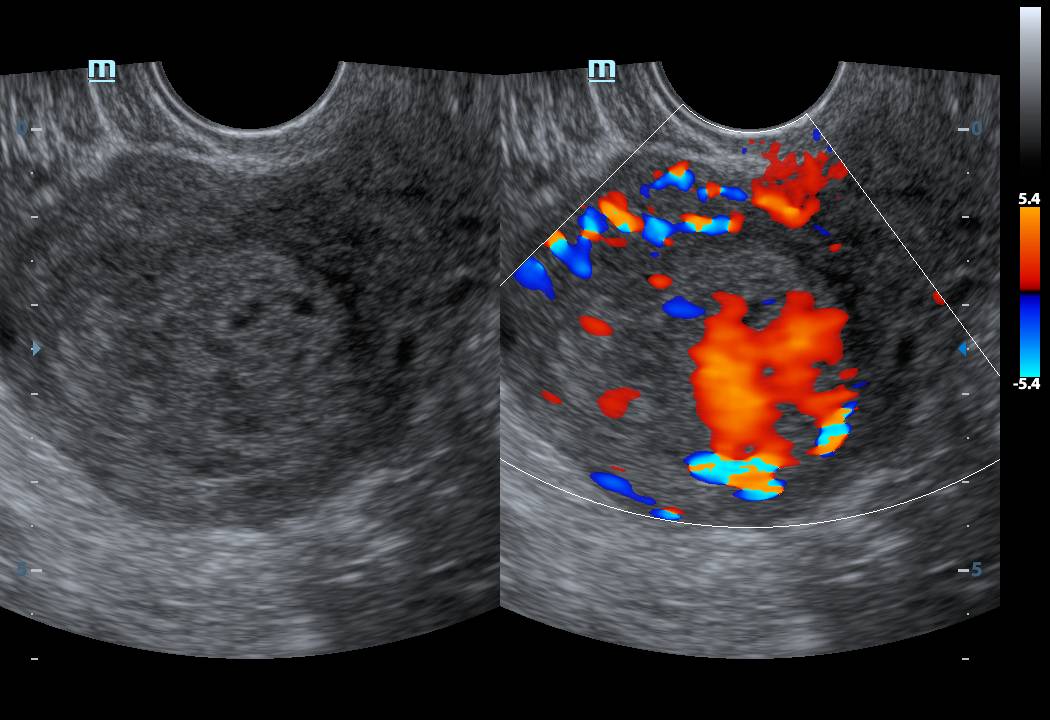
Figure 2: Presence of arterial vascularity within the mass on colour Doppler.
Figure 3 video: Echogenic intracavitory mass in the uterus with arterial vascularity on colour Doppler. There is no chaotic, multidirectional flow.
Figure 4 video: Power Doppler shows moderate vascularity in the echogenic mass.
Laboratory examination revealed the Hb to be normal, and serum beta-HCG was <0.5 mIU/mL.
Based on the clinical presentation, ultrasound and laboratory findings, a diagnosis of the placental polyp was made.
The placental polyp is a retained part of placental tissue which persists in the uterine cavity after abortion or delivery. It is firmly attached to the wall of the uterine cavity and is made up of organized villi/decidua, degenerated clots and regenerated endometrium. [1]
It takes about 4 weeks post-partum for maternal serum beta-HCG to return to non-pregnant levels. In case of a placental polyp, the level of beta-HCG tends to remain on the higher side even after 4 weeks. Thus, within 4 weeks, the beta-HCG level is not very helpful in the diagnosis of placental polyp. [2]
A close differential diagnosis is an arterio-venous malformation (AVM). The irregular vascular channels which give heterogeneous appearance to the myometrium and the chaotic, multidirectional blood flow can help differentiate an AVM, however, features of the placental polyp may sometimes overlap with that of AVM. Serum beta-HCG level is not raised in the case of AVM, which is a good differentiating point.
Loss of hypoechoic interface between the mass and the wall of the uterine cavity should raise suspicion of placental adherence.
Thus, in all cases of post-partum per-vaginal bleeding, a possibility of placental polyp must be considered. CT Angiography and MRI may also help establish the diagnosis when ultrasound is not suggestive.
© Copyright Reserved
References:
1. Shanthi V, Rao NM, Lavanya G, Krishna BA, Mohan KV. Placental polyp – a rare case report. Turk Patoloji Derg 2015;31(1):77-9.
2. Ishihara T, Kanasaki H, Oride A, Hara T, Kyo S. Differential diagnosis and management of placental polyp and uterine arteriovenous malformation: Case reports and review of the literature. Womens Health 2016;12(6): 538-43.