Fetal facial mass on ultrasound

A 25-yrs old primigravida presented for last trimester routine growth scan. The anomaly scan performed at 20 weeks was reported as normal.
The ultrasound findings were as follows:
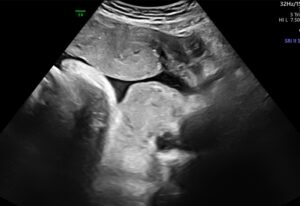
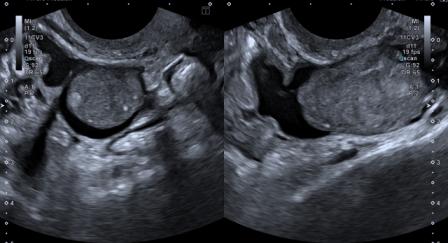
Figure 1: The coronal view of face showing soft tissue mass lesion with small cleft-like anechoic spaces. The mass was extended from lower margin of orbit to chin.
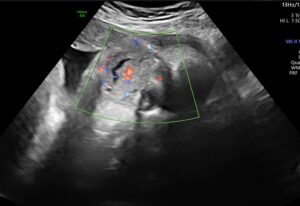
Figure 2: Colour Doppler examination shows vascularity in the mass.
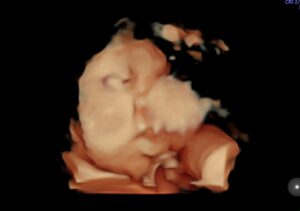
Figure 3: 3D Ultrasound clearly depicts the facial mass lesion.
Based on the ultrasound features, a diagnosis of congenital facial hemangioma was made.
Follow-up at birth and subsequently at 8 months is documented below.

Figure 4: The appearance of the facial hemangioma at birth.

Figure 5: At 8 months of age, there is significant resolution of the hemangioma.
Hemangiomas are benign vascular tumors. They can be congenital or infantile.
The natural history of a hemangioma consists of stages – initial rapid proliferation followed by stabilisation, and then, in most cases, gradual regression.
Infantile hemangiomas, which are more common, progress during the first year of life. They usually regress over the first decade. Congenital hemangiomas proliferate in-utero and reach maximum size by birth.
Following birth, congenital hemangiomas either involute rapidly or partially, or don’t involute at all.[1] Large facial hemangiomas can cause mechanical obstruction of the airway, compress or cover the eyeball, invade the cranial vault, and bleed or ulcerate. When they are very large and contain arterio-venous shunts, they can cause high output cardiac failure.[2]
On antenatal ultrasound, hemangiomas appear as solid vascular masses with abundant venous and low-resistance arterial flow. As they regress in the postnatal period, they show increasing fatty infiltration, reducing vascularity and increase in the resistance in arterial waveforms.
As compared to infantile hemangiomas, treatment options for congenital hemangiomas are limited. Rapidly involuting hemangiomas generally regress 100% by 14 months.[1]
Symptomatic hemangiomas may require resection or embolization.[3] Laser treatment and sclerotherapy may improve superficial lesions cosmetically.[3]
© Copyright Reserved
References:
1. Ramphul K, Mejias SG, Ramphul-Sicharam Y, Sonaye R. Congenital Hemangioma: A Case Report of a Finding Every Physician Should Know. Cureus. 2018;10(4):e2485. doi:10.7759/cureus.2485.
2. Weitz NA, Lauren CT, Starc TJ, et al. Congenital cutaneous hemangioma causing cardiac failure: a case report and review of the literature. Pediatr Dermatol. 2013;30:180–190.
3. Chen TS, Eichenfield LF, Friedlander SF. Infantile hemangiomas: an update on pathogenesis and therapy. Pediatrics. 2013 Jan;131(1):99-108. doi: 10.1542/peds.2012-1128.