D-TGA on fetal echo: a model demonstration

A 27-years old second gravida presented for obstetric ultrasound examination at 23 weeks 3 days gestation.
The ultrasound findings were as follows:

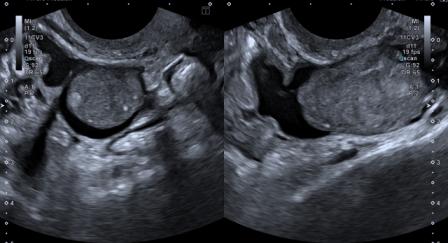
Figure 1: Apical four-chamber view shows normal atria & ventricles, atrioventricular concordance, normal insertion of tricuspid (TV) & mitral valves (MV), normal anatomic location of moderator band at the apex of right ventricle (RV) and pulmonary veins draining into left atrium. Foramen ovale appears normal.
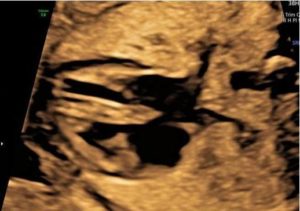
Figure 2: Intact interventricular septum.
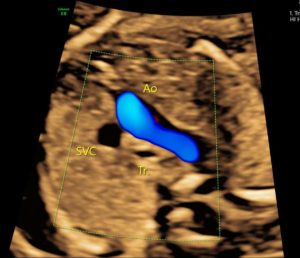
Figure 3: Three-vessel-trachea view shows only two (instead of normal three) vessels: the aorta (Ao) & superior vena cava (SVC) are seen. Pulmonary artery (PA) is not seen (due to its inferior placement).
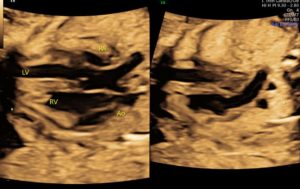
Figure 4: Five-chamber view shows complete transposition of great arteries, with Ao arising from RV and PA arising from left ventricle (LV). PA bifurcation is clearly seen.

Figure 5: Colour Doppler image demonstrating the PA arising from LV and bifurcating into right & left divisions.
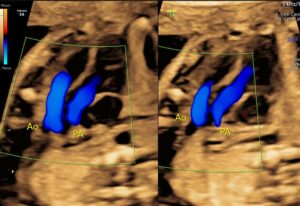
Figure 6: Color Doppler images in oblique plane demonstrating the parallel course of the great arteries, with Ao arising from RV, anterior and parallel to the PA which is arising from LV.
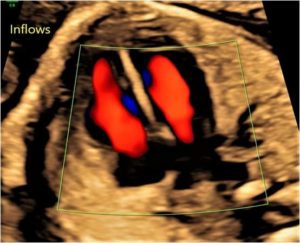
Figure 7: Colour Doppler image demonstrating normal inflow across MV & TV.
Figure 8 – Video: The colour Doppler video clearly demonstrates the transposition of great arteries.
Based on the above findings, a diagnosis of dextro transposition of great arteries (D-TGA) was made.
TGA is the result of the failure of the conotruncal septum to spiral. Instead, the septum descends straight down. This results in ventriculo-arterial discordance, with the aorta arising from right ventricle and pulmonary artery arising from left ventricle. The resultant transposition can be of two types:
1. L-TGA: Ventriculo-atrial & ventriculo-arterial (double) discordance.
2. D-TGA: Ventriculo-atrial concordance & ventriculo-arterial discordance.
Since, the circulation in L-TGA is naturally corrected (despite blood entering the wrong ventricles), it is D-TGA that is symptomatic.
Unless associated with some other cardiac anomaly like atrial septal defect, ventricular septal defect (VSD), patent ductus arteriosus or patent foramen ovale, D-TGA is incompatible with life.
More than half the cases have an intact ventricular septum, and the remaining are divided between VSD with or without pulmonary stenosis (PS).[1] VSD is typically perimembranous but can be located anywhere in the septum.[2]
Extracardiac anomalies are rare with D-TGA, and so are chromosomal anomalies.[2] However, D-TGA has been found to be associated with maternal diabetes and congenital coronary arterial anomalies.
D-malposition with double outlet right ventricle and L-TGA need to be considered in differential diagnosis of D-TGA, as all of them share the absence of “crossover” of the great vessels.
Unless indicated otherwise, delivery at 39 to 40 weeks is preferred, as last six weeks is a critical growth period.[3] At birth, in the absence of PS, volume overload in pulmonary circulation leads to variable degree of cyanosis, depending upon degree of mixing.[1] Those with sufficient PS and VSD can remain asymptomatic for some time before left ventricular deconditioning manifests.
Most hypoxemic neonates benefit from early infusion of prostaglandin E1 alone.[3] However, if the flow across foramen ovale is restrictive, balloon atrial septostomy may be required in addition to prostaglandin E1.[3] Elective arterial switch operation with or without VSD closure is the surgery of choice. In patients with significant pulmonary stenosis, temporary palliation with modified Blalock-Taussig shunt followed by a Rastelli or Nikaidoh operation may be performed.[1]
© Copyright Reserved
References:
1. Yuh DD, Varicella LA, Yang S, Doty JR. John Hopkins Textbook of Cardiothoracic Surgery, 2nd Ed. McGraw-Hill Education/Medical;2014.
2. Abuhamad A, Chaoui R. A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts. 3rd Ed. Philadephia, PA: Lippincott Williams & Wilkins;2015.
3. Villafane J, Latin-Hermoso MR, Bhatt AB, et al. D-transposition of the great arteries: the current era of arterial switch operation. J Am Coll Cardiol 2014;65(5):498-511.