Antenatal ultrasound diagnosis of choledochal cyst

A 32-years old primigravida presented for a routine antenatal ultrasound (US) for the first time at 32 weeks of gestation. Prior to this, only a dating scan had been performed.
US findings were as follows:
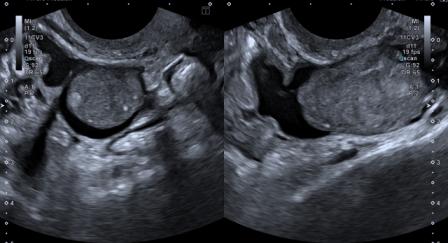
Figure 1 – Video: A well-defined, anechoic structure is seen at the porta hepatis. Gall bladder is seen separately.
Figure 2 – Video: The cystic structure at the porta hepatis does not show any evidence of intrinsic vascularity.
On antenatal US, a probable diagnosis of choledochal cyst was made, with cystic biliary atresia given as a rarer differential diagnosis.
The baby was delivered at term with normal birth weight. Postnatal US was performed, as shown below:

Figure 3: Post-natal US shows a well-defined, cystic, avascular structure at the porta hepatis, just adjacent to the gall bladder, suggestive of choledochal cyst. No evidence of intrahepatic biliary radicles dilatation.
The diagnosis of choledochal cyst on US was corroborated by postnatal MRCP. The baby remained asymptomatic and showed normal weight gain. Peri-operative cholangiogram confirmed the diagnosis of type-I choledochal cyst. Exploratory laparotomy, excision of the cyst & gall bladder with Roux-en-Y choledochojejunostomy was performed electively at two-and-half months. The post-operative course was uneventful. The baby was doing well at the last follow-up.
Choledochal cyst is a rare anomaly that appears as cystic dilatation of the extra- or intra-hepatic biliary tree. Todani et al modified the original Alonso-Lej classification to describe five types of cysts, the commonest (90-95%) being type-I choledochal cyst (cystic or fusiform dilatation of common bile duct). The earliest diagnosis on antenatal US has been reported at 15 weeks.[1]
Fetal choledochal cyst usually appears as a fluid-filled, avascular, anechoic mass in the region of the porta hepatis. Demonstration of continuity with the gall bladder or hepatic ducts or associated dilatation of intra- and extra-hepatic ducts further aids the diagnosis. Occasionally, these cysts may grow large in size and may become difficult to differentiate from other cystic lesions such as simple hepatic cyst, cystic biliary atresia, omental or mesenteric cyst, duodenal or gall bladder duplication, renal / adrenal cyst and dilated bowel loop.
Antenatal MRI may be useful when the fetal position is unfavorable or diagnosis is unclear on US.
Total excision of the cyst with adequate bile drainage is the standard treatment for choledochal cyst, since complications like cholangitis, liver cirrhosis, pancreatitis and malignancy can develop in the long-term.[1] In babies without any complications viz; dilatation of intrahepatic biliary radicles on US, elevated gamma-glutamyl-transferase and elevated direct bilirubin, surgery should be performed electively few months after birth.[1],[2] Surgery may have to be performed earlier in babies with complications.
References:
1. Spinelli M, Lavinia DM, Raio L, et al. Two-dimensional ultrasonographic prenatal diagnosis of choledochal cyst: our experience and review of literature. Gynecol Obstet Case Rep 2016;2:2.
2. Soares KC, Kim Y, Spolverato G, et al. Presentation and clinical outcomes of choledochal cysts in children and adults: a multi-institutional analysis. JAMA Surg 2015;150(6):577-84.