Bilateral ovarian hyperechoic lesions: a surprise

A 46-years old female presented for ultrasound with complaint of menorrhagia.
The ultrasound findings were as follows:

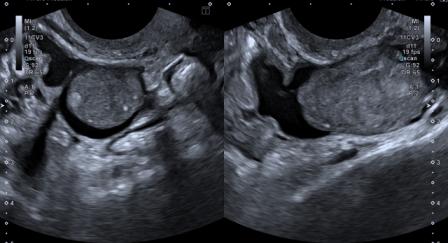
Figure 1: Transvaginal ultrasound examination revealed predominantly hyperechoic ovoid lesions in both ovaries. Intrinsic hypoechoic areas were also noted in the lesions. No evidence of cystic or calcific component.
Figure 2 – video: Transvaginal ultrasound examination shows three lesions in right ovary & one lesion in left ovary. The largest lesion in right ovary measured 3.4 x 2.8 cm, and in the left ovary measured 2.7 x 2.0 cm.

Figure 3: Power Doppler examination did not reveal any abnormal vascularity within the ovarian lesions.

Figure 4: Both kidneys showed multiple, rounded, hyperechoic lesions along the cortices, suggestive of multiple renal angiomyolipomas. Largest renal lesion was on the left side, measuring 2.6 x 2.4 cm.

Figure 5: The histopathological photomicrograph shows the ovarian lesion to be composed of mature adipose tissue, smooth muscle bundles & blood vessels. Image courtesy: Dr. Atul Bhalerao, Consultant Pathologist.
Based on the ultrasound findings, differential diagnosis of bilateral ovarian dermoids vis-a-vis ovarian angiomyolipomas (AMLs) was considered. In view of multiplicity of ovarian lesions, absence of cystic or calcific component and presence of bilateral renal AMLs, possibility of the ovarian lesions representing AMLs was considered more likely, despite the rarity of the diagnosis.
Further imaging with MRI revealed presence of fatty component within the renal and ovarian lesions. Histopathological examination of the post-surgical specimen (Figure 5) confirmed the diagnosis of bilateral ovarian AMLs.
AMLs are benign tumors, commonly affecting the kidney. While 80% of AMLs occur sporadically, 20% are associated with phakomatosis, commonly tuberous sclerosis (TS).[1] AMLs, which were earlier considered hamartomas, are now regarded part of the family of perivascular epithelioid cell tumors (PEComas), others being clear cell ‘sugar’ tumor (pulmonary & extrapulmonary) and lymphangioleiomyomatosis.[2]
Extrarenal angiomyolipomas (ERAMLs) are very rare, and the commonest sites of their occurrence are liver and retroperitoneum. The other reported sites are uterus, vagina, fallopian tube, spermatic cord, colon, abdominal wall, nasal cavity & hard palate.[2] Ovarian AMLs are exceedingly rare and thus pose a diagnostic challenge.[3]
Our patient did not have TS. Non-TS AMLs are generally small and asymptomatic. As compared to that, the TS-associated AMLs may be larger (>4cm), and may present with complications such as haemorrhage, requiring emergency embolisation.[4]
© Copyright Reserved
References:
1. Jinzaki M, Silverman SG, Akita H, Nagashima Y, Mikami S, Oya M. Renal angiomyolipoma: a radiological classification and update on recent developments in diagnosis and management. Abdom Imaging 2014;39(3):588-604.
2. Venyo AK. A review of the literature on extrarenal retroperitoneal angiomyolipoma. Int J Surg Oncol 2016;2016:6347136. doi:10.1155/2016/6347136
3. Anderson AE, Yang X, Young RH. Epithelioid angiomyolipoma of the ovary: a case report and literature review. Int J Gynecol Pathol 2002;21(1):69-73.
4. Lin C, Jin L, Yang Y, et al. Tuberous sclerosis-associated renal angiomyolipoma: A report of two cases and review of literature. Mol Clin Oncol 2017;7(4):706-8.